Neuromas & Amputation Pain
State-of-the-art microsurgery to alleviate neuropathic pain
Understanding Neuromas and Neuropathic Pain
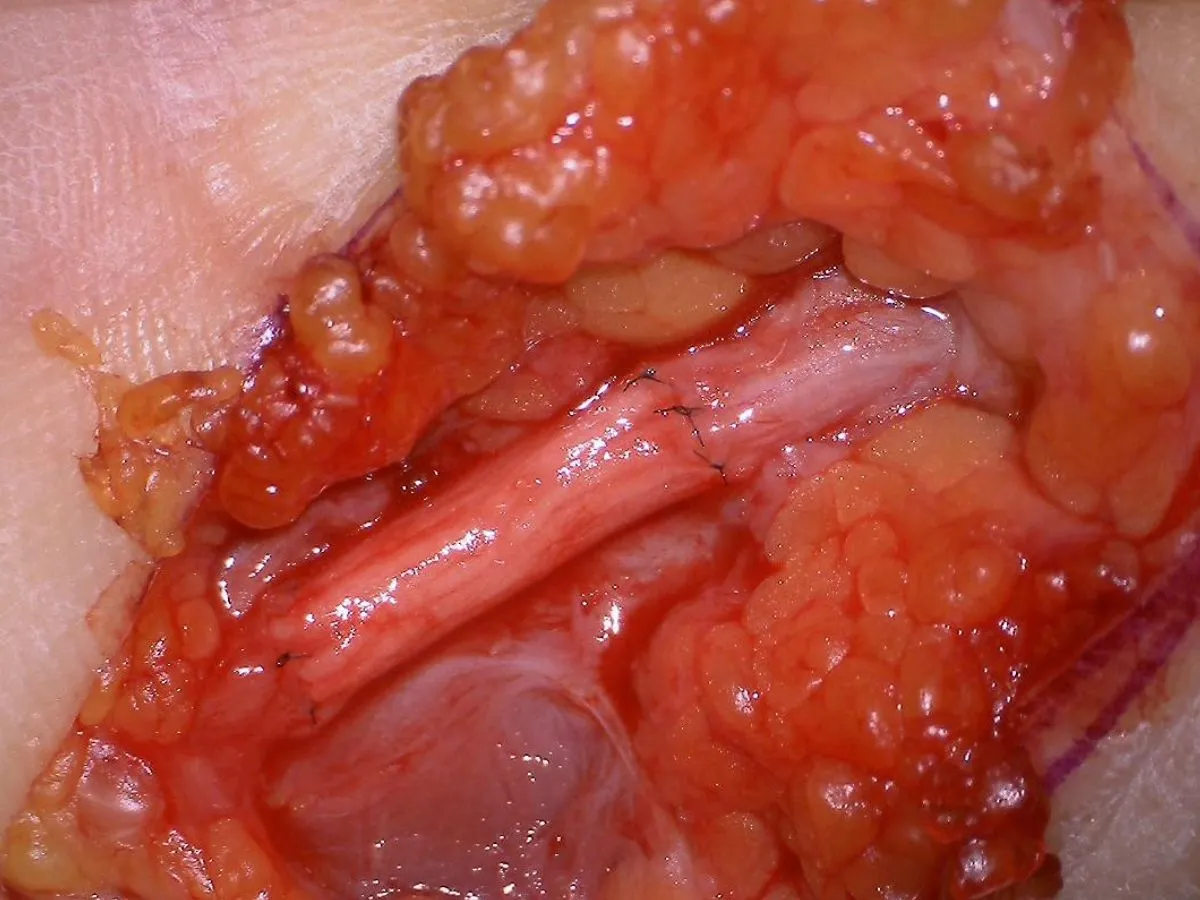
Neuromas are benign but often highly problematic nerve growths that can develop after nerve injuries, surgeries, or amputations. They occur when severed nerve fibers attempt to regenerate but cannot find their physiological target. Instead, they form a disorganized, extremely hypersensitive nerve knot.
While many neuromas remain asymptomatic, symptomatic neuromas cause severely debilitating, chronic neuropathic pain. This pain is often described as burning, stabbing, or electrifying, and can be triggered by even the lightest touch (allodynia) or exposure to cold. The persistent pain significantly impairs quality of life and leads to considerable psychosocial distress, sleep disturbances, and functional limitations.
Surgical Reconstruction and Defect Bridging
For patients where the distal (far) end of the nerve is still present, the treatment of choice is the precise surgical removal of the neuroma followed by nerve reconstruction. Restoring nerve continuity leads to significantly better clinical outcomes and lower recurrence rates than simply burying the nerve end in tissue.
- Direct Coaptation: If the resulting gap is very small, the nerve ends are reconnected directly and completely tension-free using microscopic sutures. Unfortunately, this is very rarely possible.
- Autologous Nerve Grafts: For larger defects, a sensory nerve is harvested from another part of the body (e.g., the lower leg) to bridge the gap. This is the absolute gold standard for reconstructing larger nerve defects.
- Conduits and Allografts: For shorter gaps, synthetic tubes (conduits) or processed donor nerves (allografts) can be used to protectively guide the regenerating fibers.
Innovative Solutions for Amputation Pain
Following an amputation, the severed nerve no longer has a distal target to connect to, which inevitably leads to the formation of stump neuromas. These can cause unbearable stump pain and severe phantom limb pain, making wearing a prosthesis nearly impossible.
To solve this problem, Dr. Megerle employs state-of-the-art surgical techniques aimed at giving the regenerating nerve a physiological purpose, thus preventing the formation of a neuroma:
- Targeted Muscle Reinnervation (TMR): The severed nerve is surgically rerouted into a nearby motor nerve branch of a still-functioning muscle. The nerve grows into the muscle, giving it a new "task." This significantly reduces pain. TMR demonstrates far superior results compared to traditional ablative techniques.
- Regenerative Peripheral Nerve Interface (RPNI): The nerve end is implanted into a small, free piece of the patient's own muscle tissue. This muscle graft provides a living biological target for the nerve fibers, thereby effectively and permanently preventing painful neuroma formation.

Frequently Asked Questions
What exactly is a neuroma?
A neuroma is an abnormal regeneration of nerve tissue that occurs after a peripheral nerve has been damaged or severed. Instead of reconnecting properly, undirected nerve fibers (axons) sprout into a disorganized mass of scar tissue. These nodules can become highly sensitive and cause chronic neuropathic pain.
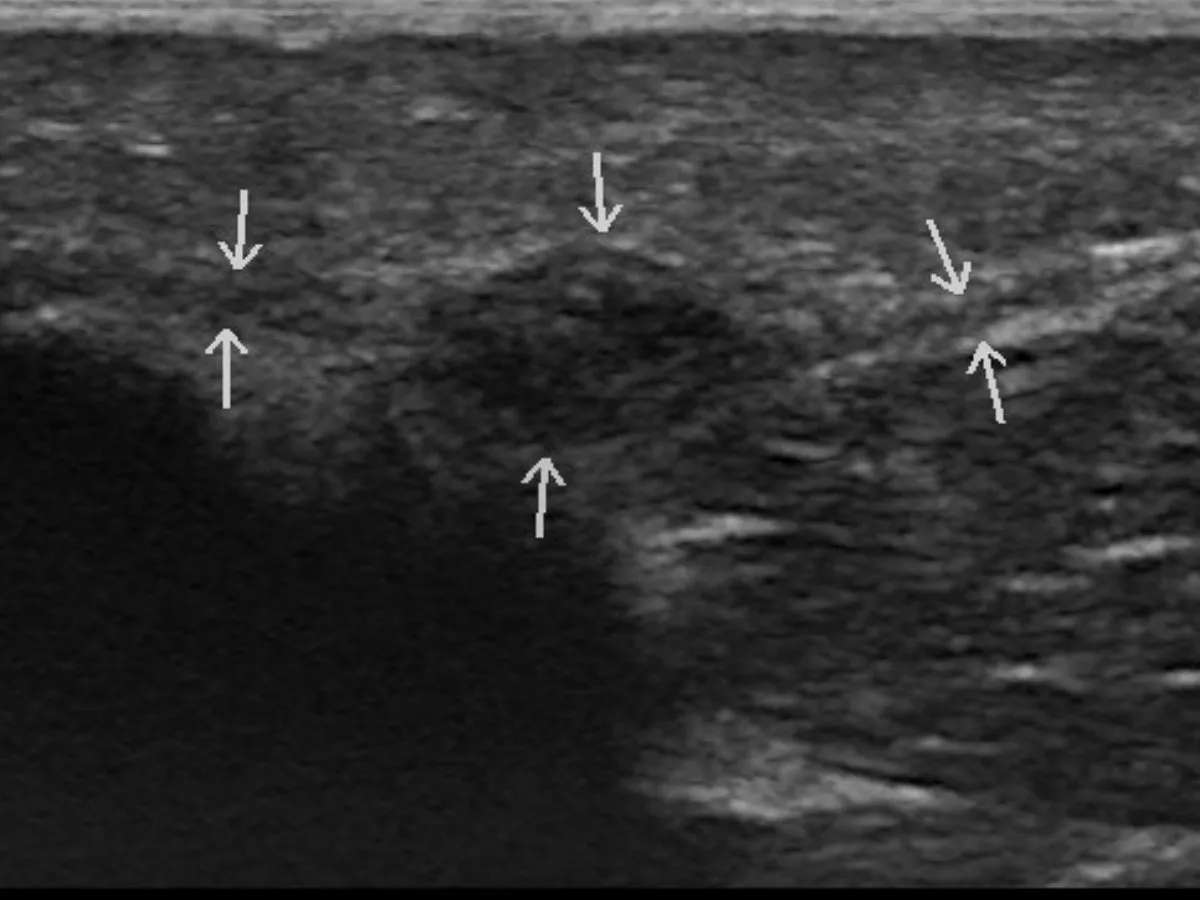
How is a symptomatic neuroma diagnosed?
Diagnosis relies on a targeted clinical examination, including the Hoffmann-Tinel sign, where tapping the nerve triggers electrifying pain. Additionally, high-resolution ultrasound can precisely localize the neuroma. Diagnostic local anesthesia blocks can further confirm the exact source of pain.
What is Targeted Muscle Reinnervation (TMR)?
TMR is a state-of-the-art surgical technique primarily used for painful stump neuromas following amputations. The neuroma is removed, and the severed nerve end is connected to a nearby motor nerve branch of an intact muscle. This gives the regenerating nerve fibers a new physiological target, significantly reducing the risk of neuroma recurrence and alleviating phantom limb pain.
What is a Regenerative Peripheral Nerve Interface (RPNI)?
RPNI is a surgical procedure in which the free end of a severed nerve is sutured into a small, free graft of the patient's own muscle or skin tissue. The tissue graft becomes engrafted and provides a biological target for the regenerating nerve fibers, effectively preventing painful neuroma formation.
Can conservative therapy help?
Yes. Before surgery, a multimodal conservative approach is often pursued. This includes specific medications for neuropathic pain (such as gabapentin or pregabalin), targeted occupational therapy for desensitization, and local injection therapies. However, purely medical therapy provides sufficient pain relief for only about 30% of patients.